
Blog
Warm Compresses for Treatment of Dry Eye

Practitioner Summary Box
⦁ To improve compliance with warm compresses, schedule patients for review appointments.
⦁ The optimal temperature for heat therapy for MGD to be between 40 and 41.5°C.
⦁ Face cloths are not effective as warm compresses unless applied using the bundle method.
⦁ Warm compress treatment is effective even without massaging the eyelids afterwards, but it is still recommended to instruct patients to massage their lids for an added benefit.
⦁ To massage the lids, instruct patient to press on the lid margin with their fingertips and to move along the lid margin until it has all been pressed.
⦁ When using an eye mask, it may take at least 2 weeks to see an improvement in symptoms and 4 to 8 weeks to see improvements in clinical signs of dry eye.
Eye care professionals are well-versed in prescribing warm compresses for dry eye treatment. However, it may not always be clear exactly what to recommend. Warm face cloths or wheat bags? For how many minutes and for how many days, weeks, or months? How much improvement can you expect? In fact, do warm compresses even work?
I will attempt to answer all these questions, based on scientific evidence, to give you some clarity and definitiveness in your recommendations and outcomes.
Do warm compresses work?
The definitive answer is yes. They most definitively do work[1-4], but they must be recommended in the right situation and for the right reasons. Warm compresses are indicated as a treatment for evaporative dry eye associated with meibomian gland dysfunction. They appear to be effective in various in varying severities of gland dropout, which adds to the importance of their use even in severe MGD[2].
Treatment with warm compresses achieves three things[5]. Firstly, it heats the meibomian gland lipids to improve their secretion into the tear film. Secondly, it reduces or eliminates meibomian gland obstruction and, lastly, it increases blood flow to tissues surrounding the meibomian glands.
Compliance
Compliance with warm compresses is one of the biggest problems with the treatment. Many patients just do not comply with their eye care professional’s treatment plan[6]. In my practice, I improve compliance by booking patients in for a review appointment. This gives the patient a target to aim for and allows me to show them how much their eyes have improved. Patients have told me that this encourages them to continue with their treatment as they know it works and that they have not been wasting their time.
Clinical Summary: To improve compliance with warm compresses schedule patients for review appointments.
Technology can help improve compliance, and you can read more about this another article I wrote here
How hot do warm compresses need to be?
Meibum naturally melts at a temperature between 32°C and 40°C[7]. In MGD, this temperature is elevated[8] as the composition of meibum is altered due to gland blockage which results in the stagnation of meibum in the meibomian glands. A recent study by Brochman found that the optimal temperature for heat therapy for MGD to be between 40 and 41.5°C[9]. That said, It is important to remind patients not to overheat warm compresses as thermal skin injury begins to occur when the skin surface temperature is maintained 45°C for 33.5 minutes[10, 11].
Clinical summary: The optimal temperature for heat therapy for MGD to be between 40 and 41.5°C
Do warm face clothes work?
A study by Olson et al. found that warm face cloths were effective at improving lipid layer thickness and tear break up in, an impressive, five minutes after treatments[3]. However, you need to look at the methods closely to see how they achieved this result. The warm face cloths were heated to 40°C, and were replaced every 2 minutes for a duration of 30 minutes. This regime is obviously not practical and is not conducive to good compliance!
Bitton et al. showed that face cloths drop to less than a therapeutic level of heat within one minute of application[12] (figure 1). The bundle method is perhaps a better option. This is a method described in a study by Murakami et al. where they bundle warm face-cloths by wrapping them in layers[1], and subsequently removing the outer most cloth to apply when the previous cloth loses heat. This video explains it well
In general, I would recommend using a facemask when possible, due its higher effectiveness. A 2014 study Sim et al. found that treatment with an eye mask to be more effective than a warm towel, and found the eye mask to be as effective as treatment with Blephasteam[13].
Clinical summary: Face cloths are not effective as a warm compresses unless applied using the bundle method.
What about wheat bags?
In my personal experience, I have found wheat bags to be a good option for patients, as many patients already have them at home, and they seem to retain heat quite well. This is based on patient feedback. In terms of scientific evidence, a recent 2020 study found that wheat bags were effective at maintaining a temperature, on the eyelid surface, of between 38 and 40 °C from the 4th to the final 10th minute of the treatment[14]. This means that if you are recommending wheat bags, you would need to ask the patient to reheat slightly at the end of the treatment and leave them on the eyes for a further 5 minutes to get a full 10 minutes of treatment at the required heat.
Clinical summary: If using wheat bags, ask patients to keep them on the eye for 10 minutes, to reheat slightly, and then place on the eye for a further 5 minutes.
What Eye Masks are recommended?
Two excellent studies that were done to answer this question are Lacroix et al. which was first and analysed the heat of the face masks themselves over a period of time, and Bitton et al. which then assessed eye lid temperature with the same masks. So the first study tells us how hot the face masks are, while the second study tells us how hot the eye lids are. The results are presented below, and they show that for all the facemasks, except the Bruder, you need to reheat the mask after about 5 minutes to keep the lids at the required temperature. The Bruder mask manages to keep the lids at the required temperature for the full, recommended treatment 10 minute treatment interval.
Clinical summary: If you are using the Bruder mask, ask the patient to just heat once and leave on the eyelids for 10 minutes. For the other masks, as them to reheat after 5 minutes.
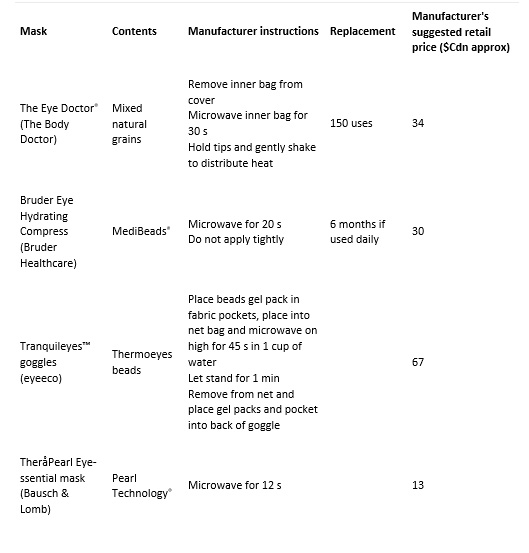
Table 1. Comparison of commercially available eyelid warming masks.[15]
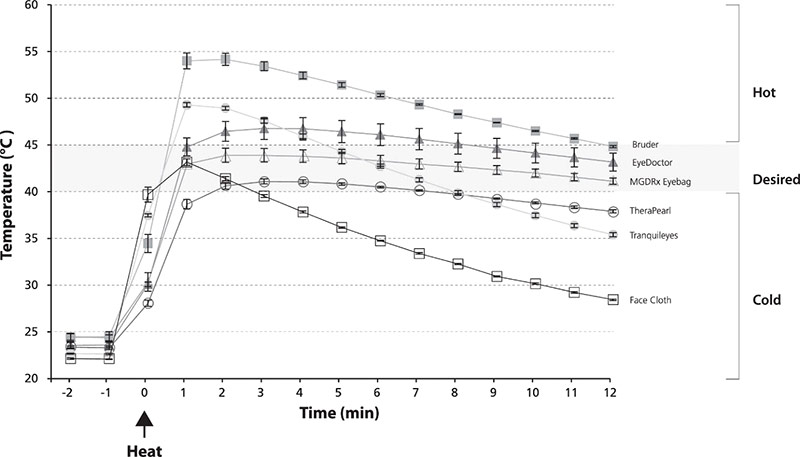 Figure 1. Heat profiles of commercial warm compresses15
Figure 1. Heat profiles of commercial warm compresses15
What is the recommended treatment duration?
When studies have found a therapeutic effect the treatment time used tends to be around 5 to 10 minutes, either once or twice a day[2, 4, 13, 16, 17]. Therefore, to be within the therapeutic range for most studies, it would be best to advise patients to do warm compresses for 10 minutes, twice a day. I find that this is a good number to aim for, as if one treatment is missed then a second is still performed. This helps to ensure a minimal level of treatment is achieved. If patients are finding it difficult to maintain treatment twice a day, this can later be reduced to 10 minutes once a day. Murphy et al. instructed their participants to apply warm compresses for 10 minutes, twice a day for 2 weeks, followed by 10 minutes once a day for the remaining six weeks of their study[4]. MGD improved significantly during the 8 week period of this study using this treatment regimen.
Do you need to press on the lid margins following the application of heat?
The short answer is no. Most studies that use warm compresses do not ask patients to massage their eye lids following application of heat. Finis et al. specifically instructed participants to massage their eyelids following heat compress application[17]. Their study found that warm compresses were comparable to Lipiflow, in improving meibomian gland expressibility, and they believed that Lane et al.’s[18] study didn’t produce similar results because the control group did not do a massage of the lid following heat application. Based on the scientific evidence though, patients will still get a therapeutic effect from warm compresses even they do not do a massage following the application of heat[2, 4, 13, 16].
Based on the weak evidence available, it is still probably recommended to ask patients to massage their eyelids following heat application. How should they do this? Fins et al. advised patients to massage their lids in the direction of the lid margin, in the upper and lower lid, using their finger tips or a cotton swap[17]. I personally find that patients get confused with this technique and massage too far away from the lid margin. I ask them to make sure that they press on the lid margin with their fingertip and to slowly move along the lid margin until they have completely covered it with their pressing.
Clinical summary: Warm compress treatment is effective even without massaging the eyelids afterwards, but it is still recommended to instruct patients to massage their lids for an added benefit.
What improvements can you expect?
Warm compresses have an almost instant therapeutic effect on the meibomian glands. Turnbull et al. looked meibomian gland function within 10 minutes of warm compress application found that lipid layer thickness NITBUT both improved significantly within this short period of time[2]. Finis et al. compared warm compresses combined with lid massage with LipiFlow, and found that the effect on meibomian gland expressibility was comparable at one month and three months[17]. However, there was no improvement in symptoms during this time. The authors did not specify what type of warm compress was used.
More recently, Murphy et al. compared the effect of warm compresses using three different warming devices – face cloths, MGDRx EyeBag, and OPTASE Moist Heat Mask[4]. The study found that only the MGDRx EyeBag®, and OPTASE Moist Heat Mask improved symptoms at 2 and 8 weeks. The OPTASE Moist Heat Mask also significantly reduced the quantity of Demodex folliculorum at 8 weeks. There was a significant improvement in MGD grade between baseline and week 8 in the EyeBag and OPTASE groups, and between week 2 and 8 in the OPTASE group only. Ocular surface staining improved between week 2 to 8 in the eye masks group. NITBUT did not improve in any of the groups.
Clinical summary: When using an eye mask, it may take at least 2 weeks to see an improvement in symptoms and 4 to 8 weeks to see improvements in clinical signs of dry eye.
References
- Murakami, D.K., C.A. Blackie, and D.R. Korb, All warm compresses are not equally efficacious. Optometry and Vision Science, 2015. 92(9): p. e327-e333.
- Turnbull, P.R., S.L. Misra, and J.P. Craig, Comparison of treatment effect across varying severities of meibomian gland dropout. Contact Lens and Anterior Eye, 2018. 41(1): p. 88-92.
- Olson, M.C., D.R. Korb, and J.V. Greiner, Increase in tear film lipid layer thickness following treatment with warm compresses in patients with meibomian gland dysfunction. Eye & contact lens, 2003. 29(2): p. 96-99.
- Murphy, O., V. O’Dwyer, and A. Lloyd-Mckernan, The efficacy of warm compresses in the treatment of meibomian gland dysfunction and Demodex folliculorum blepharitis. Current Eye Research, 2020. 45(5): p. 563-575.
- Blackie, C.A., et al., Inner eyelid surface temperature as a function of warm compress methodology. Optometry and Vision Science, 2008. 85(8): p. 675-683.
- Alghamdi, Y.A., et al., Compliance and subjective patient responses to eyelid hygiene. Eye & contact lens, 2017. 43(4): p. 213.
- Ong, B. and J. Larke, Meibomian gland dysfunction: some clinical, biochemical and physical observations. Ophthalmic and physiological optics, 1990. 10(2): p. 144-148.
- TIFFANY, J.M., The lipid secretion of the meibomian glands, in Advances in lipid research. 1987, Elsevier. p. 1-62.
- Borchman, D., The optimum temperature for the heat therapy for meibomian gland dysfunction. The ocular surface, 2019. 17(2): p. 360-364.
- Moritz, A.R. and F. Henriques Jr, Studies of thermal injury: II. The relative importance of time and surface temperature in the causation of cutaneous burns. The American journal of pathology, 1947. 23(5): p. 695.
- Despa, F., et al., The relative thermal stability of tissue macromolecules and cellular structure in burn injury. Burns, 2005. 31(5): p. 568-577.
- Bitton, E., Z. Lacroix, and S. Léger, In-vivo heat retention comparison of eyelid warming masks. Contact Lens and Anterior Eye, 2016. 39(4): p. 311-315.
- Sim, H.S., et al., A randomized, controlled treatment trial of eyelid-warming therapies in meibomian gland dysfunction. Ophthalmology and therapy, 2014. 3(1-2): p. 37-48.
- Leeungurasatien, T., A. Paungmali, and A. Tantraworasin, Efficacy of wheat hot pack (dry heat) and pottery hot pack (moist heat) on eyelid temperature and tissue blood flow in healthy eyes: a randomized control trial. International Ophthalmology, 2020: p. 1-11.
- Lacroix, Z., S. Léger, and E. Bitton, Ex vivo heat retention of different eyelid warming masks. Contact Lens and Anterior Eye, 2015. 38(3): p. 152-156.
- Arita, R., et al., Effects of eyelid warming devices on tear film parameters in normal subjects and patients with meibomian gland dysfunction. The ocular surface, 2015. 13(4): p. 321-330.
- Finis, D., et al., Evaluation of an automated thermodynamic treatment (LipiFlow®) system for meibomian gland dysfunction: a prospective, randomized, observer-masked trial. The ocular surface, 2014. 12(2): p. 146-154.
- Lane, S.S., et al., A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea, 2012. 31(4): p. 396-404.